

What are Covid-19 and the coronavirus? What are the parameters, causes and effects of this disease? What are the short and long-term prospects? Infectious disease specialist Philippe Sansonetti explains why the fate of the epidemic is in our hands.

Dossier / Faces of the Pandemic
Covid-19: Chronicle of an Outbreak Foretold
by ,
30 March 2020
translated by
|
It’s hard to believe in plagues when they fall on your head.
– Albert Camus, The Plague

This text is taken from the conference given by Philippe Sansonetti at the Collège de France, 16 March 2020
Covid-19 is a plague, and it is vital that our society realise this as a matter of urgency. It is not too late, but we are running out of time.
This is the third outbreak of a coronavirus in the past twenty years, after SARS in 2003 and MERS in 2012. Each of these incidents left people worried, then reassured, and not much happened thereafter to predict and anticipate such incidents occurring again in terms of treatment and vaccines. Now, in the absence of treatment and vaccines, the progression of this epidemic is in our hands.
Charles Nicolle (1866-1936), a professor at the Collège de France and director of the Pasteur Institute in Tunis, wrote in Destin des maladies infectieuses (1933):
There will thus be new diseases. It is a fatal fact. Another equally fatal fact is that we will never be able to detect them at their very source.
Knowledge of infectious diseases teaches us that we have to come together in solidarity. We are brothers under threat from the same danger, united by the fact that the contagion is more often than not passed on to us from our fellow men. In this respect, and regardless of our feelings towards them, we are also in solidarity with animals, and domesticated animals in particular.
A foretaste, then, of all of the outbreak phenomena that would occur in the 20th and now 21st centuries.
What is a coronavirus?
Coronaviruses are a huge family of single-stranded ‘positive’ RNA (ribonucleic acid) viruses, meaning that this RNA is expressed directly in the form proteins that form both the structure of the virus and its entire replication and multiplication engineering systems. This is a very large family and one with which we live on a daily basis, since alpha-coronaviruses are found in mammals, including humans, and can cause benign respiratory and intestinal diseases, particularly in children. In this respect, there is nothing new about the aetiology of this type of disease. The problem is that other coronaviruses belonging to this family and known as beta-coronaviruses are rather well-adapted to mammals, notably including the bat, which is the primary reservoir of the disease, but are not very well adapted to humans, meaning that when they do transfer to humans we see conflict and damage as a result of this encounter between a micro-organism and a host that are not well adapted to dealing with one other. Other members of the family, known as gamma and delta-coronaviruses, are found in birds and fish and have not, for the time being at least, given us any cause for concern in terms of an outbreak.
Identifying the virus
We must also point out the positive aspects of what is currently happening, aspects that can sometimes be overlooked. The first of these is the very unusual speed with which this epidemic was first detected in the Chinese city of Wuhan, as soon as doctors noticed a number of strange cases of pneumopathy, some of which were already severe. Diagnoses that even ten or twenty years ago would have taken weeks or even months to make since the virus had to be isolated and identified were now being established using molecular methods in just a few days or even hours, thanks to the development of so-called new-generation deep sequencing and bioinformatics, which made it possible to identify this foreign RNA immediately in samples taken from these infected individuals and to develop a specific amplification system for these viruses in real time in order to make a very quick diagnosis and launch epidemiological studies. This could be compared with the months or even years it took to identify the AIDS virus thirty years ago, when the virus had to be cultivated using classical virological methods. Molecular diagnosis has revolutionised the situation, and despite some initial delays in awareness and communication regarding this epidemic, the Chinese doctors and biologists concerned can be praised for successfully identifying the virus as quickly as they did.
The pandemic spread of the virus
The situation progressed rapidly from ’clusters’ to a nationwide epidemic, and the problem now is no longer blocking borders or implementing any other archaic ideas; the borders now are right there on our own front doorsteps. The map showing how active outbreaks of the pandemic have spread shows something of a belt corresponding to the latitudes of our European regions (and the corresponding regions of the southern hemisphere, such as Australia) and for the time being relatively few cases in the southern countries of the intertropical zones. Some attribute this effect to our climate, and it would be nice if that were true, as this could mean that with “warmer temperatures in the spring”, as Donald Trump puts it, things may get better, but there is certainly no solid scientific grounding to this. There are, however, probably a number of other reasons that are not yet clear, and I will come back to these later.
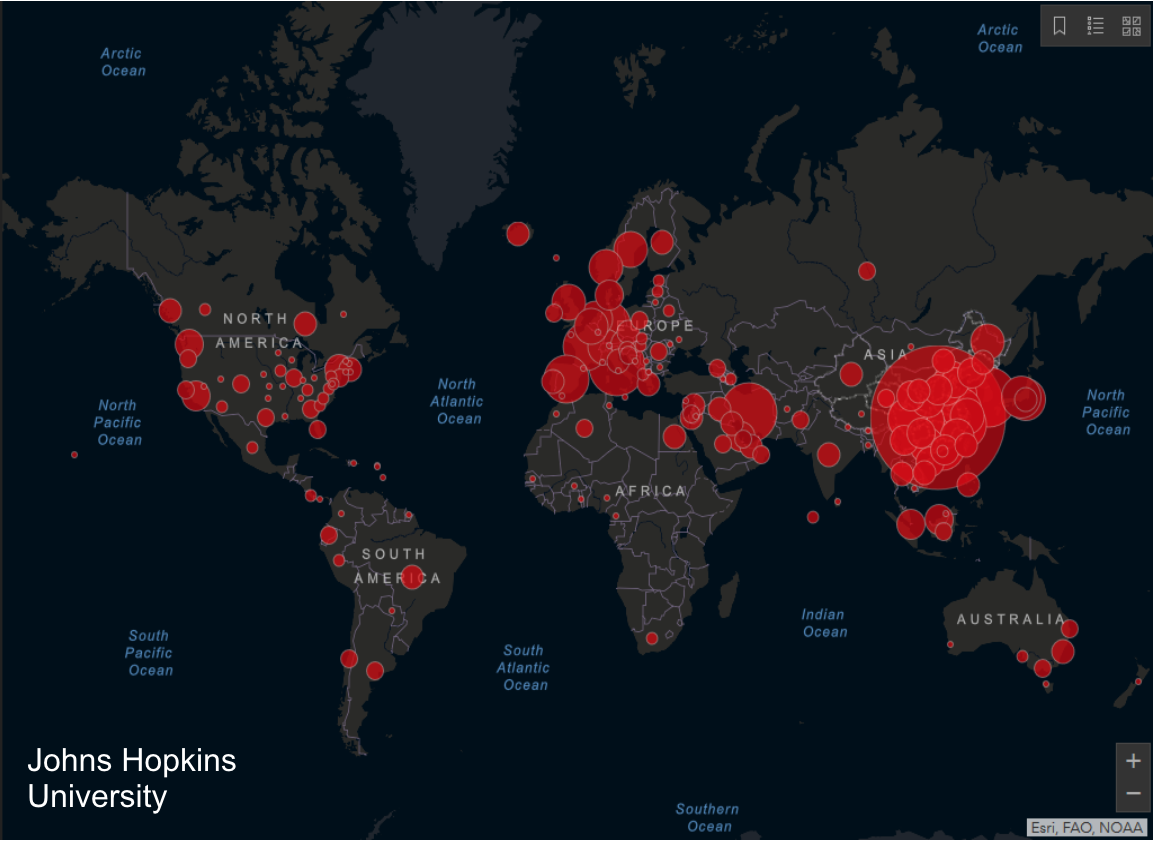
Extension pandémique du Covid-19 : Monde
14 mars 2020: Monde (123 pays), 145000 cas et 4026 décès.
What it is is a pandemic, meaning that we are no longer looking for patient zero or recognising the channels of transmission.
The parameters of the epidemic
What are the parameters of the disease dynamics ? The R0 (basic reproduction number) is the average number of secondary infections produced when an infected individual is introduced into a population where all individuals are susceptible. Provided that the R0 remains below 1, there is no epidemic situation; as soon as it rises above 1, this is classed as an epidemic. In the case of Covid-19, this number stands somewhere between 2 and 3, making it a typical epidemic situation. The Spanish flu of 1918-1919 had an R0 of 2-3, with tuberculosis having an R0 of 10, making it extremely contagious, and the figure for measles rising to between 12 and 18.
The incubation period is 5 to 6 days, although the virus can incubate for up to 14 days, hence the isolation period required. The intergenerational interval, that is the time between an infected individual encountering a treatment-naive (completely untreated) individual and the latter developing the disease, is 4 to 7 days. The fact that these two parameters are almost identical shows that, contrary to what happened with SARS in 2003, where contagion only manifested itself at the peak of viraemia after several days’ progression, patients are, in this case, contagious from the outset. Here, on the contrary, the virus is very highly contagious, with people transmitting despite still being asymptomatic or starting to experience minor symptoms that do not bother them when they should, in actual fact, already be self-isolating as soon as possible.
The attack rate (that is the number of newly infected individuals in relation to the total naive population) is much higher than that of seasonal flu. By definition, we do not yet have figures regarding the percentage of the French population that may actually be infected.
In severe cases, which account for around 10 to 15% of those affected, the average hospitalisation period is around 11 +/- 4 days (between 7 and 15 days), which, as we know, poses a threat to our healthcare system.
The disease therefore has a high epidemic potential, putting the health system under great strain, and this is what has prompted the authorities to introduce a series of strategies for limiting the progression of the disease, and justifiably so.

The mortality rate
The mortality rate is relatively low and is expected to eventually stand at 1-2% once we have a comprehensive overview of the pandemic. It appears higher during periods of epidemic acceleration, as is currently the case in France, not necessarily because diseases are more severe during this time but simply because we are chasing the figures; mortality figures are indisputable, whilst the figures for individuals infected with the virus are always much higher than what is observed. Specialists in the United Kingdom claim that there are likely to be 10 times more infected individuals than confirmed cases, especially since there is no doubt that in the vast majority of cases the individual will experience a mild form of the disease, making it extremely difficult to establish an accurate mortality rate. This mortality rate could, however, increase in the situation we are currently experiencing of increased strain on the medical system and the availability of intensive care beds. A mortality rate of 1% and a severe case rate of 10% may not appear to be that alarming statistically, but in relation to the number of cases of infection, given the transmissibility and infectiousness of the virus, it does go some way towards achieving the sorts of absolute values that could put our healthcare system at risk, mean that such a mitigation policy is entirely justified.
Interspecies transmission and human responsibility

Coronavirus
The name coronavirus comes from the S protein (S for spike) that connects to the receptor and is crown-like in shape on the surface of the virus, particularly where lung tissue is concerned.
The phylogenetic tree shows that SARS-CoV-2, the official name of the Covid-19 virus, very closely resembles the SARS and MERS viruses of 2003 and 2012 respectively and the diseases are, in fact, very similar. Their origins are also close, with bats found to be the reservoir of the coronavirus. We are therefore relatively familiar with this field, and the progress made with previous diseases can be applied here, even though, unfortunately, no vaccines or other forms of treatment have been developed as a result.
Covid-19 is a textbook example of an infectious outbreak caused by interspecies transmission (‘zoonosis’). For decades now we have been witnessing these sorts of zoonoses, particularly in tropical regions (as was the case with Ebola, for example) and have established that they are viruses that have adapted to animal species and that are then transmitted to the human species, meaning that there are various potential scenarios.
It could be that the virus is poorly adapted and finds it difficult to mutate and therefore to adapt in order to stabilise itself. Human infection is abortifacient, meaning that adaptation is poor and there will be no human-to-human transmission; the process will stop in the first individual affected. The process can, however, lead to potentially serious diseases, as was the case with avian influenza H5 N1, caused by direct transmission from birds to humans, with a very high mortality rate of around 60% but with no human-to-human transmission.
Other viruses, on the other hand, are better adapted to this transmission from animals (and mammals in particular) to humans from the outset, and the enzyme that replicates this strand of RNA makes a lot of mistakes, resulting in mutations that increase the chances of the virus adapting. This was the case with SARS-CoV-2, which passed relatively easily from bats to humans via a mammal, which served as an intermediate reservoir, making this a typical case. The disease was more severe and the mortality rate higher with both SARS (10%) and MERS (35%). In this case, the virus causes fewer serious illnesses but this is counterbalanced to some extent in that since it is less aggressive it is also more transmissible, and this balance is crucial to determining the disease profile.
The natural reservoir has been found to be certain species of bats, and it is impressive to see to what extent these animals are capable of carrying these emerging viruses, such as the coronaviruses. This is likely to be the case with Ebola, and the Nipah virus in Malaysia that appeared in the late 1990s, whereby changes in ecological conditions caused by human behaviour results in these bats coming into contact with animals that are themselves susceptible to this interspecies transmission and can replicate the virus. This creates a risk zone around humans since any contact between man and these reservoir animals could potentially result in the disease transferring to and consequently infecting humans. In the case of the SARS outbreak of 2003, it is believed, based on highly circumstantial evidence, that the intermediate animal was, rather than the bat, the webbed civet—a feline particularly common in Asia (and originally in the Himalayas)—, whereas in the case of MERS it is believed to have been the camel.

Pangolin
This is not specific to coronaviruses, either. In the case of Ebola, the cycle likely involves the great apes, the problem lying solely in human-to-human transmission once interspecies transmission has occurred. In the case of SARS-CoV-2, the animal in question is thought to be the pangolin (formerly known as the anteater), with numerous studies showing that the virus very closely resembles the one observed in humans, and the trafficking of these animals shows that these emerging diseases are the result of human behaviour. Indeed, it is estimated that around a million pangolins have been transported from their African homes to Asia because Asian communities are fond of both their meat and their scales. The human component plays a role in all emerging diseases; these small animals were sold under the counter at this fish market in Wuhan and that is where people initially became infected.
Some 70% of the traders operating at markets selling civets were testing positive for coronavirus in the aftermath of the SARS epidemic. Clearly, then, there are permanent areas where interspecies transmission can occur and sometimes, because the virus has mutated and acquired a small additional genome fragment, it suddenly becomes perfectly adapted for transmission to humans, meaning that we are constantly under threat from these emerging diseases. These are anthropocene diseases that are primarily, if not exclusively, linked to the fact that humans are taking over the planet and to the impact that man is having on the latter.
What goes for the climate and the environment also goes for infectious diseases, especially emerging ones, and the three factors are linked, giving us a three-part story: 1/ accidental interspecies transmission, 2/ potential overflow, if the interspecies transmission meets the relevant criteria and humans can be infected and transmit the virus to other individuals, and 3/ pandemic explosion as a result of intercontinental transport. The map showing sources of infection and the map of intercontinental flights (of which some 4 billion were made in 2019) overlap entirely. The role transport plays in the transmission and spreading of these epidemics, which then become pandemics, is therefore perfectly clear. Then, of course, there may be environmental aspects, including temperature changes in southern regions and perhaps also a delay in diagnosis, but the comparison between flights and sources of infection is striking.

Pandemic explosion as a result of intercontinental transport.
The eco-pathology of beta-coronaviruses
The SARS-CoV-2 and 1 coronavirus receptor is an enzyme that attaches to the surface of the cells, including those in the lungs, pneumocytes, endothelium, endocardium, kidney, liver and intestine. It is, of course, odd to think that a virus would select the angiotensin II-converting enzyme, an important enzyme in regulating blood pressure and the one that maintains the vascular pressure that creates blood pressure, as a receptor.
This may explain the severity of the disease, which can include potentially severe pneumopathy in the ultimate form of acute respiratory distress syndrome (ARDS), as observed in rather elderly subjects aged 60 and over and in those with chronic co-morbidities, such as diabetes, arterial hypertension, cardio-respiratory deficiency and chronic immuno-suppression, leading to oedema and destructive inflammation of the pulmonary alveoli, resulting in a need to resuscitate. The virus does affect the alveolar-capillary barrier, that is the interface for the exchange of oxygen between the cells of the pulmonary alveolus responsible for circulating oxygen from the inhaled air and the red blood cells of the pulmonary capillaries. Damage to this system results in respiratory problems that will eventually require resuscitation.
The signs of this aggravated form of the disease are the classic inflammatory signs, the so-called ‘cytokine storm’, which involves a significant increase in proinflammatory cytokines and chemokines. What is less classic, however, is this ARDS and the corresponding destruction of the alveolar-capillary barrier, which is rare but does require rapid intervention in order to supply oxygen to the body. ARDS can also occur in younger, recovering individuals, which may be linked to the body’s immune response.
Virus-specific adaptive immune responses are, however, still poorly understood. We know that the virus is quite stubborn and that it tends to annihilate this immune response, which it likely ‘learned’ to do in bats, but we do not know why or what effectors are involved.
The future is in our hands
The future of this Covid-19 pandemic is in our hands. We have the ability to prevent and to treat the symptoms of severe forms, but that is all we have for the time being. Current preventive measures are based on this new notion of social distancing (whereby everyone maintains a distance of at last a metre from anyone else, etc.) and personal hand hygiene, which I want to emphasise; of course, contamination can occur through exposure to droplets emitted by infected patients sneezing or coughing. It seems, however, that in the vast majority of cases, contaminated hands are the real vector of the disease, either through contact with an infected patient or indirectly through contact with a surface onto which these droplets have been deposited and on which the virus seems to be able to survive for several hours. It is important, therefore, to avoid hugging and shaking hands, observe the highest standards of hand hygiene and avoid touching your face until you have washed your hands or cleaned them using hydro-alcoholic gel. We must take the utmost care in this respect and remain vigilant at all times in order to protect both ourselves and the community.
The aim now is the flatten the epidemic curve in order to protect our health system and avoiding overburdening it with seriously ill people. The problem is that the measures that have been outlined so far have clearly been insufficient, as we have seen in the case of Italy, meaning that we will need to isolate and stay home, which makes sense given the intrinsic dynamics of the epidemic. We must be aware of the severity of the situation. It is easy to think that it will not happen to you. The only good news is that children of 0 to 9 years of age are not affected, but collective effect is very significant. The world as we knew it has changed dramatically in just a few days, and we must change the way we operate in order to adapt to this new reality. We must weigh up the things we valued in the past, our day-to-day activities, our leisure time and our work, against the severity of the situation, and the right thing to do in the immediate future is, unfortunately, to reduce our activity levels and isolate people as much as possible. The further the epidemic progresses, the more difficult or even impossible it will be to control and the more we will be forced to let things take their course. Now is the time to take action. There are still too many careless members of the population showing they have failed to adopt the right attitude over recent days. The message has not yet not got through to them.
Our health authorities are left with three main options:
1/ The first—which may appear somewhat cynical—would be to take the approach that the more individuals that are infected, the easier it will be for the population to gain immunity, bringing the epidemic to a natural end owing to a lack of immunologically naive individuals. This forms the basis of the concept of herd immunity. To put a figure on it, if 60% of the population were infected, the epidemic would stop because the virus would be unable to circulate within the community, but the price we would pay for this would be a very violent but relatively short-lived epidemic that would result in a staggering number of severe cases, as observed during the Asian flu epidemic that hit the United Kingdom in 1957. The health system imploded for a week to ten days as health workers became sick and owing to a lack of adequate equipment, resulting in a huge number of serious cases.
2/ The ‘Chinese approach’, which is the complete opposite and involves the blanket isolation of both towns and cities and individuals and seems to be effective in undeniably controlling the epidemic. The risk, however, is that few individuals will have been infected (as a result of a lower attack rate due to confinement) and the majority will remain naive to the virus, meaning that the virus is likely to return in an epidemic rebound, thus justifying their fears of the disease returning from currently infected areas such as Europe, hence the absolute necessity of a vaccine to prevent such potential rebounds.
3/ The middle ground approach that we have adopted, which involves flattening the epidemic curving and spreading it out over time in hope that a little under 60% of the population will eventually be infected and, above all, that the entire health system will be protected as a result. It is hoped that in addition to this we will see the evolutionary engineering of infectious diseases that Charles Nicolle spoke of at work, enabling us to pull through the epidemic, but it is still very difficult to make predictions about how long the episode might last. One thing for sure is that the epidemic is primarily in our hands.
Treatment
In addition to trying to prevent it, it is vital that we find anti-viral treatments to help reduce the severity of certain forms of the disease and even to block person-to-person transmission if widespread use were possible. This will require us to first ‘reposition’ certain drugs already proven to treat other viruses (such as HIV), followed by others that are more specific to the virus in question and ultimately any others that might follow.
There is also an urgent need to better understand the pathophysiology of ARDS in order to develop a dedicated pharmacology using repositioned molecules and eventually completely new molecules.
These diseases, like Covid-19, are among the emerging diseases we are likely to see in the future, and it is vital that an effective vaccine be found. The corresponding design, research & development, validation and clinical study stages and registration with the relevant regulatory agencies all take between 8 and 12 years for a standard vaccine, which is, of course, incompatible with the urgency of an outbreak. The ability to identify new vaccine targets has improved considerably over recent years and we already have candidate vaccines that are going to start entering the clinical trial phase and will be managed in a way that accelerates the process as much as possible. That said, we know that all this will take at least a year and will only allow us to manage the rebounds and the final stages and even to prevent the disease on other continents such as Africa, where isolation measures would be difficult to implement. The vaccine is essential, and will involve all parties, including the Institut Pasteur, the Inserm, etc., but the scientific development will take time and in the meantime, during this otherwise empty phase, it is down to us to take our fate into our own hands in terms of the way in which we understand this disease and the need for these isolation measures and stricter individual hygiene practices. It is not every day that one event has such a profound impact on our fate. Infectious diseases are certainly forming the basis of modern warfare and our lives are undoubtedly going to change as a result of this.
Dossier(s) :
Faces of the Pandemic
Faces of the Pandemic
by , 30 March 2020
Share this article
Find us here :


Further reading
Transcript: A. Suhamy
To quote this article :
Philippe Sansonetti, « Covid-19: Chronicle of an Outbreak Foretold », Books and Ideas , 30 March 2020. ISSN : 2105-3030. URL : https://laviedesidees.fr/Covid-19-Chronicle-of-an-Outbreak-Foretold
Nota Bene:
If you want to discuss this essay further, you can send a proposal to the editorial team (redaction at laviedesidees.fr). We will get back to you as soon as possible.
You might also like




Our partners


Sections
Keep in touch
© laviedesidees.fr - Any replication forbidden without the explicit consent of the editors. - Mentions légales - webdesign : Abel Poucet